ALSO READ: 10 principles of the fertility diet
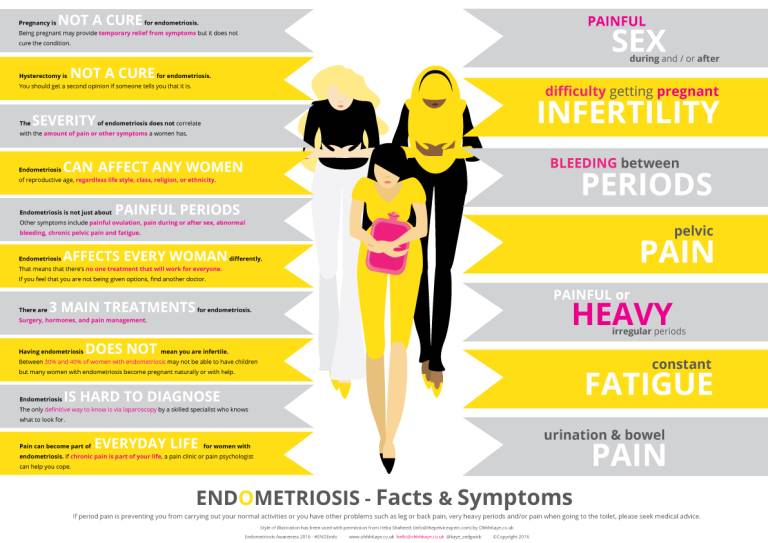
Endometriosis is a disorder where tissue similar to the lining of the uterus is found elsewhere in the body. This tissue can be found on the ovaries, fallopian tubes or the intestines. It can present with symptoms of women having severe pain in their lower abdomen, pain during menses, pain during sex or on passing stool and inability to conceive.
Inspired by her experience with endometriosis, Doris Murimi founded the Endo Sisters East Africa Foundation. She opens up about the condition and how it is being handled in Kenya.

What inspired you to start EndoSisters?
Endo Sisters East Africa Foundation (EndoSisters) was born out of my pain and struggle with undiagnosed endometriosis for 30 years. As devastating as it was to be diagnosed with endometriosis, there was a great sense of relief in finally labelling what I had been going through. It proved to me that I was not crazy, and most of all, that the pain was real – it was not imagined.
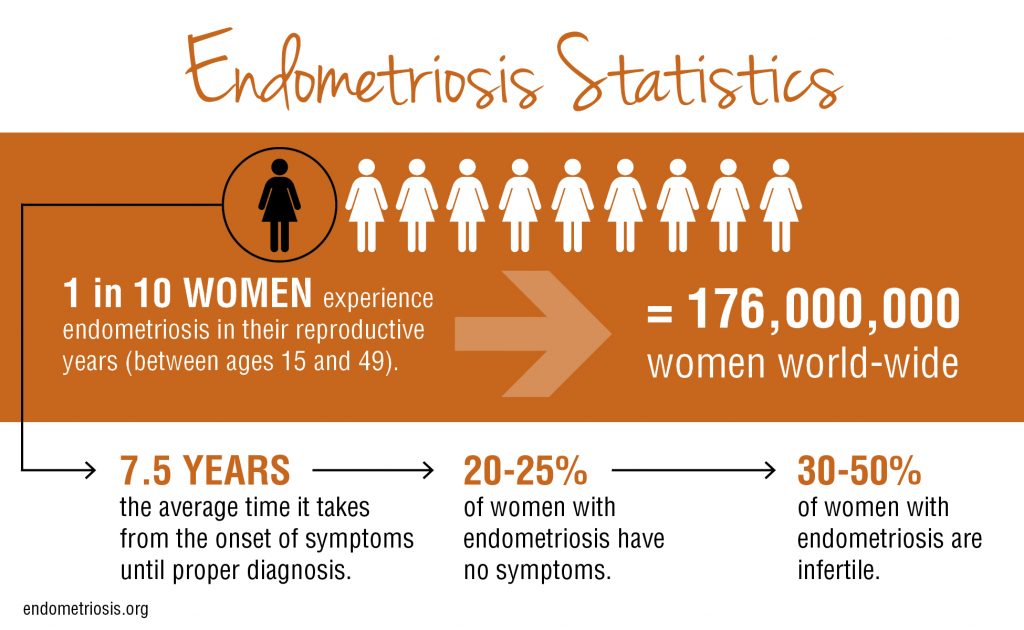
Following my diagnosis, I googled the word ‘endometriosis’ as I had never heard of it. Approximately one out of every 10 women of childbearing age have endometriosis and 176 million women worldwide live with endometriosis.
I was really devastated when I learnt that there was no cure and that it only got worse with age. My symptoms included pelvic pain, heavy and prolonged menstruation as well as pain with bowel function, and intestinal pain. I suffered from chronic fatigue and low back pain. When menstruating, it would experience diarrhoea, nausea, dizziness and bloating. It went on to include pain down the sciatic nerve also known as leg endometriosis. The fact that I also had fibroids added to the low self-esteem as well as depression I was experiencing.
ALSO READ: How diet affects your sex health
Due to this, I felt like a big part of my life had been taken over by endometriosis leading to such poor quality of life. It reached a point where I could no longer work. However, I did not want that to be someone else is story. I wanted them to have a better narrative with a better outcome than me particularly through early diagnosis. In this respect, my focus has primarily been adolescents as I wish someone had told me about endometriosis during my teens when I started experiencing those symptoms.
What is the scope of EndoSisters? What do you deal with?
We are a social advocacy organization conducting community awareness activities. We do this in support of the legal and natural rights of women living with endometriosis and other menstrual disorders as a means to achieving social justice.
Our mission is to share information, educate, collaborate, advocate, and encourage women suffering from endometriosis and related ailments (infertility and other menstrual disorders).
What are some of the worst cases that you have come across so far?
Obviously one of the worst cases would be Njambi Koikai’s case which is Thoracic endometriosis. Additionally, the progression of endometriosis is incredibly fast these days that we are seeing girls of 24- 26 years with advanced endometriosis, infertility and other complications.
Many of them had been initially misdiagnosed and have had symptoms for 5 -7 years. I think this is pretty devastating for the young ladies when their adult life is just beginning. The other category is that endometriosis appears to come with an additional condition in some women. In my case it was fibroids, other women its adenomyosis, and there are those who get all three conditions (endometriosis, adenomyosis and fibroids). Last year, we lost one of our group members and friend who had both adenomyosis and cancer (myeloid leukemia
ALSO READ: 12 things you should know about the intrauterine device (IUD)
How does the Foundation spread awareness and provide support to women?
We believe that early diagnosis is critical in mitigating the progression of endometriosis and enhancing the quality of life for adolescent girls and women. Undiagnosed endometriosis can cause untold gynaecological complications, infertility, and psychological trauma and may pre-dispose a patient to a particular kind of ovarian cancer (particularly where there is family history of cancer). Unfortunately, there is no cure for endometriosis.
For More of This Stories Subscribe to the Standard Epaper to get a copy of Eve Woman in the Standard

Has the government helped in any way?
The cost of treatment is very expensive and totally out of reach for many adolescent girls and women. This is because the hormonal medications given are not covered by insurance as they are deemed to be fertility enhancing medications yet they are the recommended course of treatment for endometriosis and other ailments.
The case to be made for inclusion is that in line with Universal Health Care (UHC), investing now in adolescent/female health care through provision of essential prevention and treatment services, enables the Ministry of Health’s (MoH’s) response to improve the quality of girls and women’s’ lives, in addition to reducing long-term health and economic costs.
In my perspective, the Government through MoH should:
In terms of diagnosis
MoH to ensure that every level 5 hospital across the 47 counties must have a laparoscopy equipment for the diagnosis of endometriosis. They should partner with other training institutions such as Institute of Primate Research and have gynaecologists receive training on the use of the laparoscopy tower to enable proper diagnosis. MoH should provide funding for gynaecologists to receive laparoscopic trainings. And finally, MoH should ensure that laparoscopy surgery should also be covered under the National Hospital Insurance Fund (NHIF) as a diagnostic tool and also during treatment.
In terms of treatment
MoH to ensure that endometriosis is recognized as a non-communicable disease (NCD) to qualify for subsidized medication and treatment through NHIF as it is done for example for cancer medication. A case in point is a drug called Zoladex which is used in the treatment of both cancer and endometriosis. This drug is accessible for free through NHIF for cancer patients but not for endometriosis patients who are prescribed for the same medication.
Some women also receive it as a treatment for fibroids reduction. Zoladex is a relatively expensive drug and so are other GnRH drugs. Also, MoH to ensure that for women with a diagnosis of infertility or who are at a high risk of infertility due to advancement of endometriosis and other menstrual disorders, have access to procedures such as egg stimulation, egg freezing and IVF covered under NHIF. The lack of coverage for fertility issues is a real financial burden and an area that traumatizes women and couples who are affected.
In terms of psychosocial interventions
MoH under NHIF should allow for counselling visits/sessions to enable girls and women have access to professional services that will enable them cope with their condition. They should also provide financial support for existing psycho-social support groups that walk with these women to enable provision of psychosocial support.
In terms of awareness creation
MoH should organize campaigns to promote national awareness of endometriosis. Carrying out information campaigns on the social and economic impact of endometriosis can change the way women manage their health, well-being, and working life and the way they are treated by society. Endometriosis awareness should be included in the formal Kenyan education system under menstrual health given that the onset of the condition begins as early adolescence. Inclusion in the education curriculum will really help in awareness, early diagnosis and in the mental well-being of affected girls by reducing stigma, anxiety, self-esteem and ensure that school performance is not negatively affected. MOH should bring the Ministry of Education on Board as a partner to ensure this endeavour is actualized.
In terms of research
MoH to fund and conduct countrywide epidemiological and socio-economic study about endometriosis and its consequences. This is a critical step toward raising awareness about this unknown illness, collecting essential data, and collating the necessary evidence on the social, health, and economic implications of endometriosis.
What is your vision as an organisation? What do you hope to see become a reality?
We want to see an environment in Kenya where endometriosis is included in the reproductive health agenda. This should be evidenced at the very minimum by the availability of gynaecologists’ (qualified to undertake laparoscopic surgery) in each of the 47 counties level 5/6 hospitals.
The output is expected to be increased access (number of women accessing medical care) and lowered costs (consultation, medication, and laparoscopy) in respect to endometriosis treatment and management in Kenya.
What are the everyday struggles women deal with while living with endometriosis?
The quality of life of a woman/adolescent girl living with endometriosis is so impaired. Research has shown that endometriosis affects 10 percent of women in the reproductive-age group. This increases up to almost 50 percent in patients with infertility.
Endometriosis has a negative impact on marital/sexual relationships, social life, and on physical and psychological aspects in all the affected women. It also impacts education for young women aged between 16–24 years, life opportunities and employment for women between 25–34 years while those aged 35 years and above face negative financial impact.
The economic burden of this disease is also high and similar to other chronic diseases such as diabetes, Crohn’s disease and rheumatoid arthritis. To compound it all, girls whose mothers or close family members have endometriosis are 5-7 times more likely to have endometriosis.
What is the heaviest/hardest part of your job?
The frustration of not being able to provide financial support to women and adolescent girls that need to access treatment. It is really depressing especially because we understand just what they are going through. It is the reason why we continue to engage the MoH (Division of family Services).
What would you advice someone who suspects she might be having endo or any menstrual condition?
I would advise them to see a gynaecologist immediately to obtain an early diagnosis. It could be endometriosis, another menstrual disorder or nothing at all, but better safe than sorry.
What about parents/guardians/caregivers whose daughters are experiencing extremely painful periods in their teens? What should they do, where should they go?
The first step is to take your daughter to a see a gynaecologist once she starts menstruating particularly if she is complaining of pain. In addition to doing a physical exam, the doctor will take her medical history by asking her about any concerns and symptoms she has. Parents/guardians should encourage their daughters to keep a pain and symptoms diary that details what she experienced at different times during her cycle so that it can inform the doctor’s course of action.
This month, EVE is focusing on reproductive health, you can follow the conversation and content on https://www.standardmedia.co.ke/evewoman/topic/reproductive-health.
Are you suffering from endometriosis, fibroids or PCOS? You can share with us or send your questions on [email protected] or inbox us on Facebook (@evewoman) or Instagram (@evewomankenya).
Do not miss out on the latest news. Join the Eve Digital Telegram channel HERE.